

Cognitive Content – WS
Skill Title :
Wound Suturing
LEARNING OBJECTIVES:
- Indications for Suturing
- Equipment required for suturing.
- Simulators For Suturing
- Procedure for suturing
- Complications associated with suturing
INTRODUCTION :
A suture is a stitch or series of stitches made to secure the apposition of the edges of a surgical or traumatic wound. This closure method is a means of primary repair of skin and deeper layers (subcutaneous tissue, fascia, etc.) to promote wound healing. The suture material is an artificial fibre used to keep the edges of the wound together until they hold themselves naturally.
INDICATIONS FOR SUTURING
- Clean wounds with little skin loss that can be closed with little strain/ tension.
- Securing drains/lines to prevent loss (e.g. central lines, intercostal drains)
- Operative closure
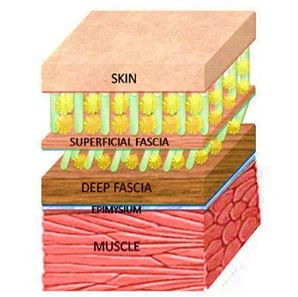
ANATOMY OF SKIN AND FASCIA
The skin is the body’s outermost protective layer and consists of three primary components: the epidermis, dermis, and subcutaneous tissue. The epidermis acts as a barrier against external threats, the dermis provides structural support, and the subcutaneous tissue houses blood vessels and fat, contributing to insulation. Beneath the skin lies the fascia. Fascia consists of connective tissue. The fascia attaches, stabilizes, imparts strength, maintains vessel patency, separates muscles, and encloses different organs. Fascia can be classified as Superficial, Deep, Parietal and Visceral.
Proper suturing of the fascial layer is crucial in surgeries to promote tissue approximation and prevent complications. When suturing, it’s essential to consider the anatomy of these layers carefully, ensuring meticulous closure to promote optimal wound healing and minimize the risk of infection or other post-operative complications.
SELECTION OF SUTURES AND BASIC SUTURING TECHNIQUES
TYPES OF SUTURES:
- Absorbable Sutures:
These sutures break down naturally over time and are commonly used for internal tissues. Examples include polyglycolic acid (PGA), polylactic acid (PLA), and polydioxanone (PDO) sutures. - Non-Absorbable Sutures:
These sutures do not degrade and are often used for skin closure or in situations where long-term tissue support is required. Examples include silk, nylon and polyester.
BASIC SUTURING TECHNIQUES:
- Interrupted Suture:
This is the most common procedure used for closing a wound and the technique is mentioned in the given procedure.
In this technique, individual stitches are placed independently, securing wound edges. It provides precise control and minimizes tension at the wound site.
- Continuous Suture:
Also known as a running suture, this method involves a single, continuous thread passing through the wound, allowing for a quicker closure. However, if one part of the suture fails, the entire line may loosen.
- Simple Interrupted Suture:
Each stitch is tied individually. This technique is versatile and suitable for most wounds.
- Mattress Suture:
This technique includes both deep and superficial layers of tissue. It provides excellent wound edge approximation and is particularly useful for areas under tension.
- Subcuticular Suture:
Typically used for cosmetic purposes, this method involves suturing just below the skin surface, leaving no visible suture marks.
EQUIPMENT REQUIRED FOR SUTURING
- Sterile Gloves
- Suture Kit: needle holders, forceps (ideally toothed- Adson’s forceps) & scissors
- Povidone-iodine or chlorhexidine solution
- Appropriate suture (size/material/needle)
- Saline
- Gauze/ Cotton
- Local anaesthetic: With or without adrenaline (e.g. 1% Lidocaine with 1:200000 adrenaline)

SIMULATORS FOR SUTURING
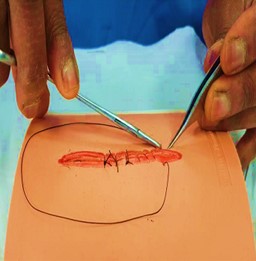
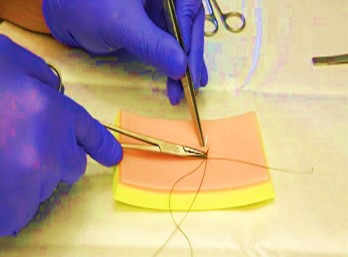
PROCEDURE FOR SUTURING ON SIMULATOR
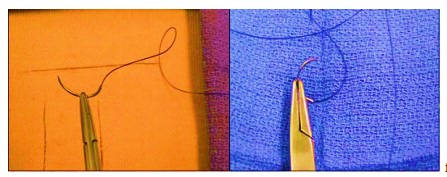
Technique for Needle Orientation:
- Grasp the suture needle one-third the distance from the swage between the tips of the needle driver.
- Hold the needle perpendicular to the long axis of the needle holder.
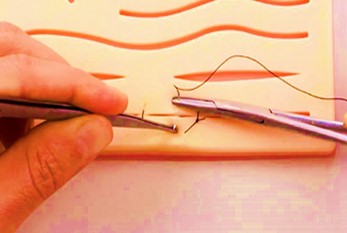
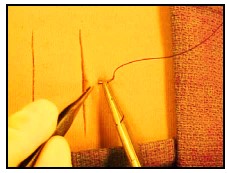
Technique for Simple Interrupted Suturing:
- Using Adson forceps for skin retraction, insert the needle tip into the tissue approximately 0.5 cm to 1 cm from the wound edge, making sure to begin with the needle perpendicular to the tissue surface.
2. Supinate the wrist clockwise 90 degrees to facilitate needle passage through tissue. The needle should traverse the epidermis, dermis, and a small portion of subcutaneous tissue.
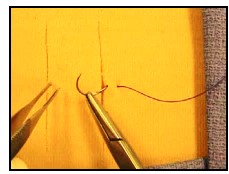
3. Grasp the needle within the wound (avoid grabbing the tip, as doing so will dull the needle). Secure the needle with the forceps, grasp it with the needle holder, and rotate the wrist clockwise 90 degrees to complete needle passage through the tissue.
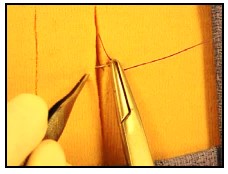
4. Using Adson forceps for skin retraction, insert the needle tip into the subcutaneous tissue of the opposite wound edge.
5. Supinate the wrist clockwise 90 degrees such that the needle exits the skin 0.5 cm to 1 cm from the wound edge.
6. Secure the needle with the forceps, grasp it with the needle holder with palms facing down and a supinate wrist, rotating the needle through the skin.
7. Secure (tie) the knot using a two-handed technique (prerequisite) after removing the needle from the suture to approximate wound edges without undue tension
8. Cut the suture, leaving a 1 cm tail on the suture.
9. Space simple, interrupted sutures approximately 1 cm apart.
COMPLICATIONS OF SUTURING:
- Dehiscence
- Infection without dehiscence
- Suture reactions
- Ligature loop failure
Comments